| Flexor tendon ruptures are most often due to either sudden trauma, attrition from chafing against a sharp bone prominence, or a combination of both. Flexor tendon ruptures within the carpal tunnel are most often due to attrition from the latter cause, with two common patterns. Protruding osteophytes of the radius, scaphoid or trapezium are the culprits for radial tendon ruptures, such as the flexor pollicis longus. Nonunion of a hook of hamate fracture is a likely etiology for a small finger flexor tendon rupture in the carpal tunnel. The etiology is not always clear, as illustrated by this case. |
| Click on each image for a larger picture |
| This elderly gentleman presented with a six week history of inability to flex his small finger, interfering with his golf game. This problem developed suddenly after unexpectedly striking a root during a golf swing. He had no active flexion of either interphalangeal joint. He denied bruising or pain and had no tenderness. Differential diagnosis included flexor tendon rupture at the profundus insertion or within the carpal tunnel due to a hook of hamate nonunion. |
 |
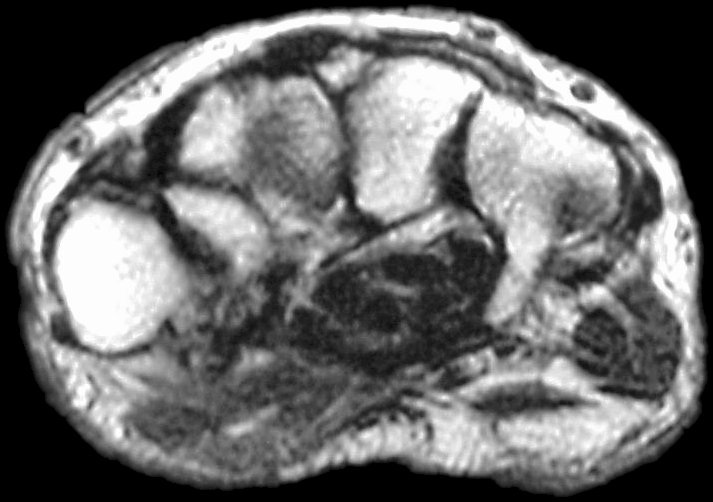
| Mild wrist stiffness prevented adequate visualization of the hook of the hamate with plain films. Plain films of the finger were normal for age. Further evaluation was obtained with MRI. Flexor tendon signals in the finger were normal: |
 |
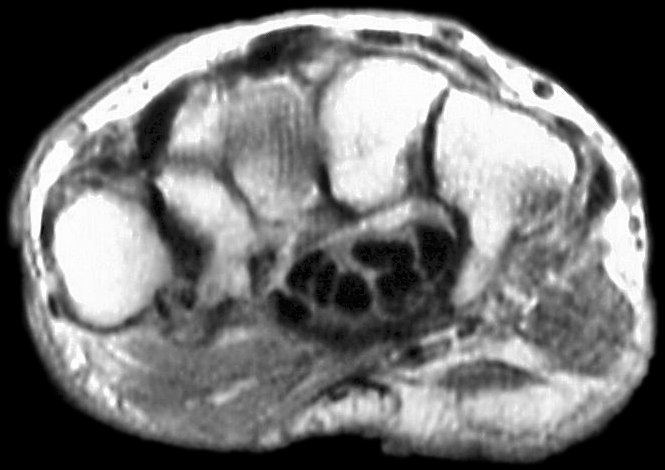
| Sections through the carpal tunnel - looking for a hook of hamate fracture or tendon discontinuity - were read as normal, although there may be a subtle signal irregularity through the hook of the hamate: |
 |
 |
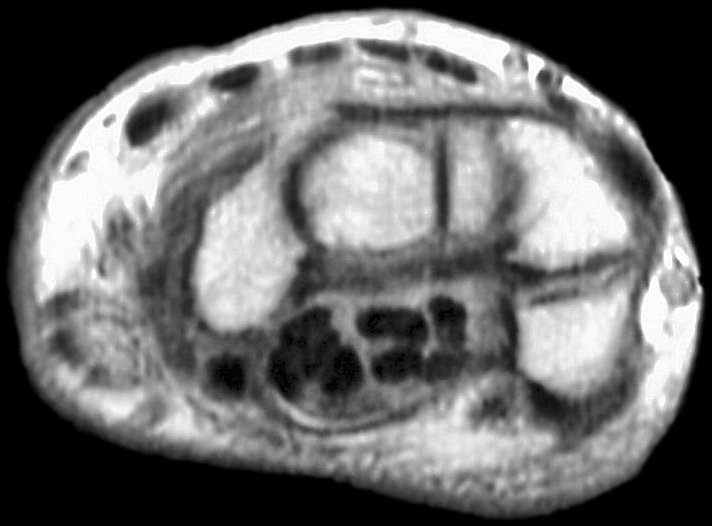
| Is that a tendon rupture adjacent to the pisotriquetral joint? |
 |
 |
 |
 |
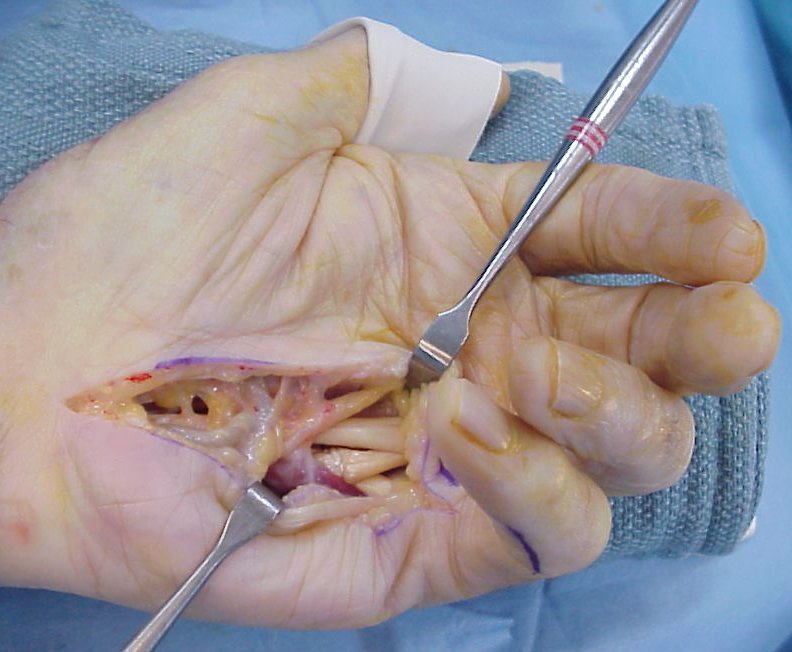
| The diagnosis was flexor tendon rupture, site uncertain. He was explored and found to have ruptured both flexors of the small finger within the carpal tunnel: |
 |
| Thorough exploration of the hook of the hamate and pisotriquetral joint were remarkable only for what appeared to be loss of soft tissue cover of the radial cortex of the hook of the hamate. No fracture line was identified, but because of this abnormality, the hook of the hamate was removed. The small profundus was reconstructed with an end to side weave to the ring finger profundus tendon: |
 |
| Postoperatively, the patient did well, and returned to playing golf. |
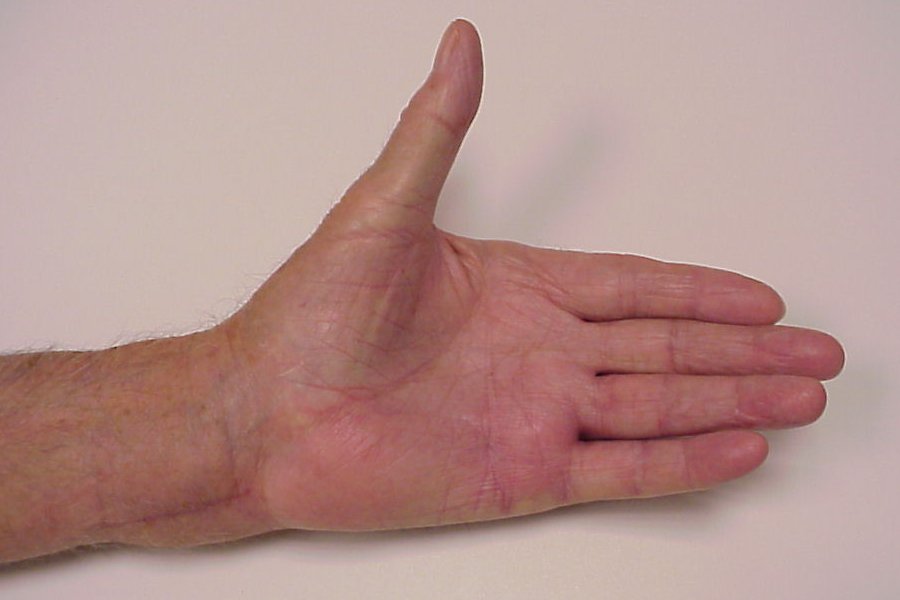 |
| This picture demonstrates full range of motion. |
 |
| However, the truth is that despite careful intraoperative technique, he lost full flexion of the ring finger distal interphalangeal joint, due to either scarring or imbalance of the tendon transfer tension. Pictures can be misleading. Fortunately, his golf swing was unaffected, and he was pleased with the result. |
 |
| Search for...
flexor tendon rupture hamate complication attritional tendon rupture |
Case Examples Index Page | e-Hand Home |